December is make-or-break for Mother Jones’ fundraising. We have a $350,000 goal that we simply cannot afford to miss. And in "No Cute Headlines or Manipulative BS," we explain, as matter-of-fact as we can, how being a nonprofit means everything to us. Bottom line: Donations big and small make up 74 percent of our budget this year and are urgently needed this month, and all online gifts will be matched and go twice as far until we hit our goal. Please pitch in if you can right now.
December is make-or-break for Mother Jones’ fundraising, and in "No Cute Headlines or Manipulative BS," we hope that giving it to you as matter-of-fact as we can will work to raise the $350,000 we need to raise this month. Donations make up 74 percent of our budget this year, and all online gifts will be matched and go twice as far until we hit our goal.
Here’s the coronavirus death toll through April 26. The question of the day is: Why am I using data from the COVID Tracking Project for recent US death tolls? What’s wrong with the Johns Hopkins data?
Nothing, really. But here’s the thing: everyone’s mortality data is probably wrong. Evidence from analysis of excess deaths—that is, the number of deaths each day this year compared to the same day last year—suggests that we’re counting COVID-19 deaths wrong. The actual death toll is probably 50 percent higher than the official numbers. Maybe more.
But that doesn’t matter too much when you’re looking at trendlines. As long as the counting method is wrong in a consistent way, you’re OK. Unfortunately, a couple of weeks ago New York City decided to adopt a new counting procedure and they suddenly added 3,700 new COVID-19 deaths to their previous toll. This wasn’t because more people had actually died. It was solely because they changed the way they count.
If you use the new number, you get a big, artificial spike in the overall US number that doesn’t represent anything real. So I decided that in order to keep the trendlines readable, I’d use the overall number from the COVID Tracking Project, which doesn’t include New York’s spike. That’s why my number is different from the one you see on the news every day.
The raw data from Johns Hopkins is here. The COVID Tracking Project is here. The Public Health Agency of Sweden is here.
Birx said the task force intends to continue working with states to scale up testing for those sick with the virus. “At the same time,” she added, “we have to realize that we have to have a breakthrough innovation in testing” for those who have already had the virus but had either mild or no symptoms.
Say what? There’s no way to do enough testing with our current PCR-based tests? “We have to be able to detect antigens,” Birx said. We need a “huge technology breakthrough.”
Todd followed up. There’s really no way to ramp up testing capacity using the current PCR tests? No, no, not at all! You’ve misunderstood! Birx then said something about new technology that will come online “in the next two to three weeks.” The antigen testing is just better and easier.
Hell, I can almost see how Donald Trump could get confused if this is how his advisors talk about things. We could obviously ramp up testing using currently existing technology if we wanted to. It might be expensive and it might take a while, but it’s just a manufacturing and infrastructure task and Congress has allocated $25 billion to it. That’s a lot of money!
So why this initial blather about how we really can’t ramp up testing without an antigen screening tool? Beats me. And what is this new PCR testing technology that’s coming online in the next few weeks? I’ve read about lots of new testing tech, but I don’t know which one Birx is talking about. Or is she just guessing that one of them is bound to pay off sometime soon?
This is nuts. If there’s one thing that literally every expert seems to agree on, it’s the need for vast amounts of testing capacity. This is why Democrats added that $25 billion to the recent coronavirus bill. So why can’t we ever get a straight answer from anyone in the Trump administration about just what the plan is? This isn’t the Manhattan Project, after all, and it’s not something that needs to remain a secret from the public. Just tell us.
The World Health Organization would like to retire the phrase “social distancing” in favor of “physical distancing.” Their logic is impeccable: viruses are transmitted when you get physically close to another person, not when you’re chatting on FaceTime or holding a virtual meeting on Zoom. As long as you’re physically separate, you should feel free to be as social as you want.
Fine. But that got me curious: who came up with phrase social distancing in the first place? Does it go back to the 1918 flu pandemic, when physical distancing and social distancing were more or less the same thing, so no one cared about the distinction? Or what?
This turns out to be surprisingly hard to get a handle on. I am, obviously, talking about social distancing as a phrase that refers to a way of fighting epidemics. I don’t care about crinoline skirts or the social habits of the 16th century Spanish court. The concept of social distancing as a way of keeping your inferiors in their place goes back quite a ways.
But in the current epidemiological sense, it doesn’t seem to go back even to the start of the century:
The first use in the New York Times comes in 2006: “If the avian flu goes pandemic while Tamiflu and vaccines are still in short supply, experts say, the only protection most Americans will have is ‘social distancing,’ which is the new politically correct way of saying ‘quarantine.’ ”
The OED has a reference from the Detroit News from 2004:
I’ve found a few other brief references going back to the SARS epidemic in 2003, though none give any hint to the origin of the phrase.
And the Google Ngram Viewer, fascinatingly, shows two jumps in the use of the phrase. The first obviously refers to some kind of sociological phenomenon and started gaining popularity in the early 70s. The second, which is almost certainly SARS-related, began in 2004 and then took off in 2005.
So circa 2003 it is, unless someone comes up with something better. But who coined the phrase? And why did they choose to call it social distancing? In 2003 there was obviously a world of difference between social and physical distancing. Is there anyone out there who wants to take the blame for this?
Alex Tabarrok is unhappy about the amount of money we’re spending on R&D to fight COVID-19:
The latest relief bill contains another $320 billion in small business relief and $25 billion for testing. Finally, we get some serious money to actually fight the virus. But as Paul Romer pointed out on twitter, this is less than half of what we spend on soft drinks!!!….Despite monumental efforts by BARDA and CEPI we are also not investing enough in capacity for vaccine production so that if and when when a vaccine is available we can roll it out quickly to everyone (an issue I am working on).
The failure to spend on actually fighting the virus with science is mind boggling….Are we more politically divided about PCR tests than we are about unemployment insurance? I don’t think so yet we spend on the latter but not the former. The rot is deeper.
I want to push back on this a little bit. Not completely, though: Generally speaking, I think the evidence suggests there really has been something of a slowdown in the related areas of American entrepreneurship and innovation over the past few decades. But I’m not sure it’s as bad as it’s sometimes made out to be.
First off: spending on COVID-19 testing isn’t R&D. We already have the tests. It’s just infrastructure and technology spending. It is disgraceful that we’ve been so slow to roll this out, but it’s not really related to R&D.
Ditto for vaccines. There are something like 70 or 80 vaccine trials in process right now across the globe and something like 20 or 30 of them are happening in the US, a number fantastically higher than we’ve ever attempted before. But the gating item is mainly testing, not money. There might be something I’m missing here, but I don’t think increased spending is really an issue. As for production of vaccines, that’s more than a year away and I don’t really doubt that funding will be there when we need it.
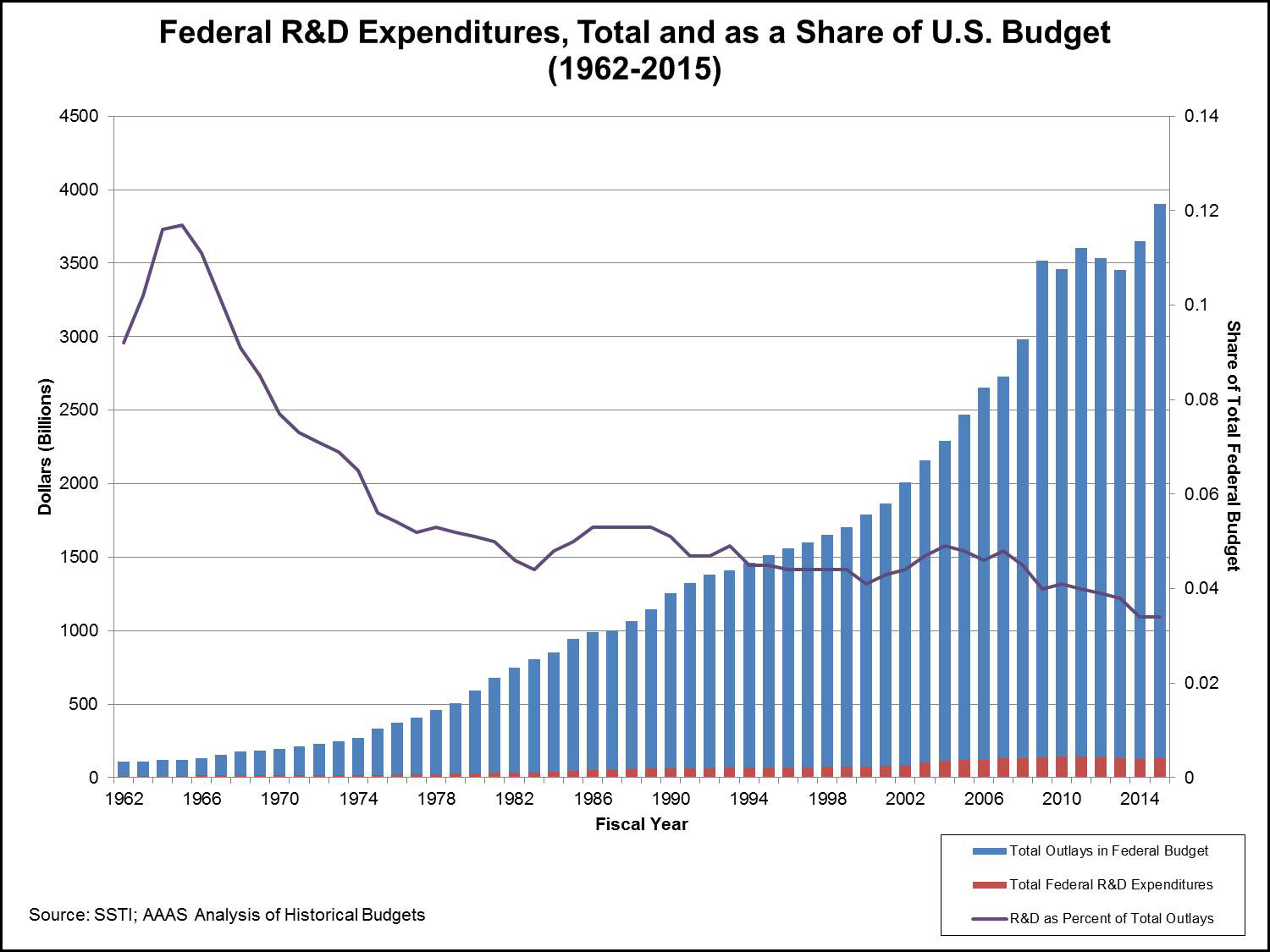
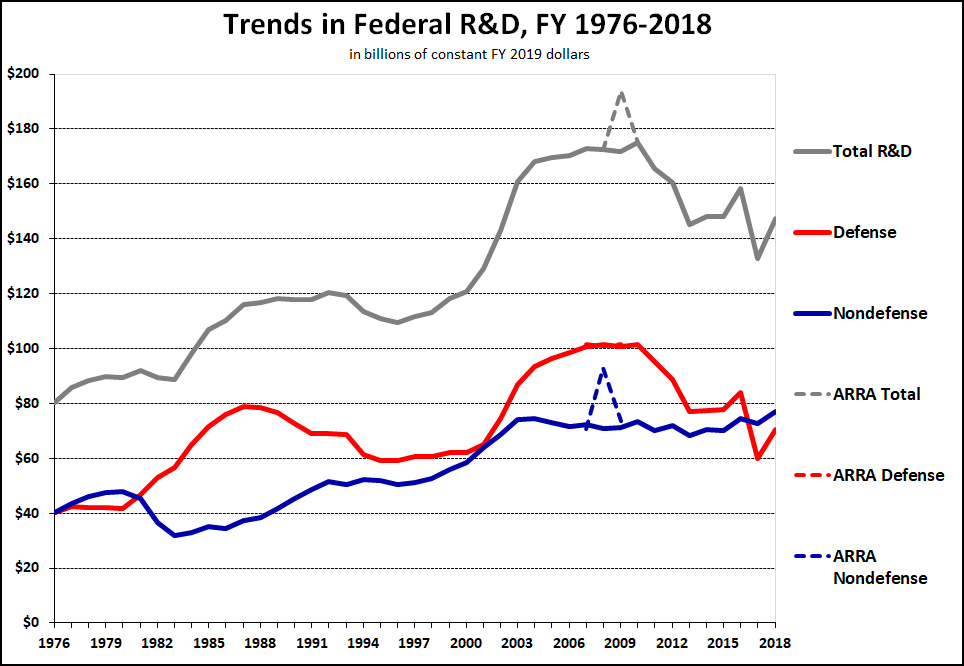
Finally, Tabarrok’s chart shows a slow decline in federal R&D spending as a share of the federal budget, but who cares about that? What matters isn’t whether we’re spending money on other stuff, but the absolute amount we’re spending on R&D. So here’s another chart:
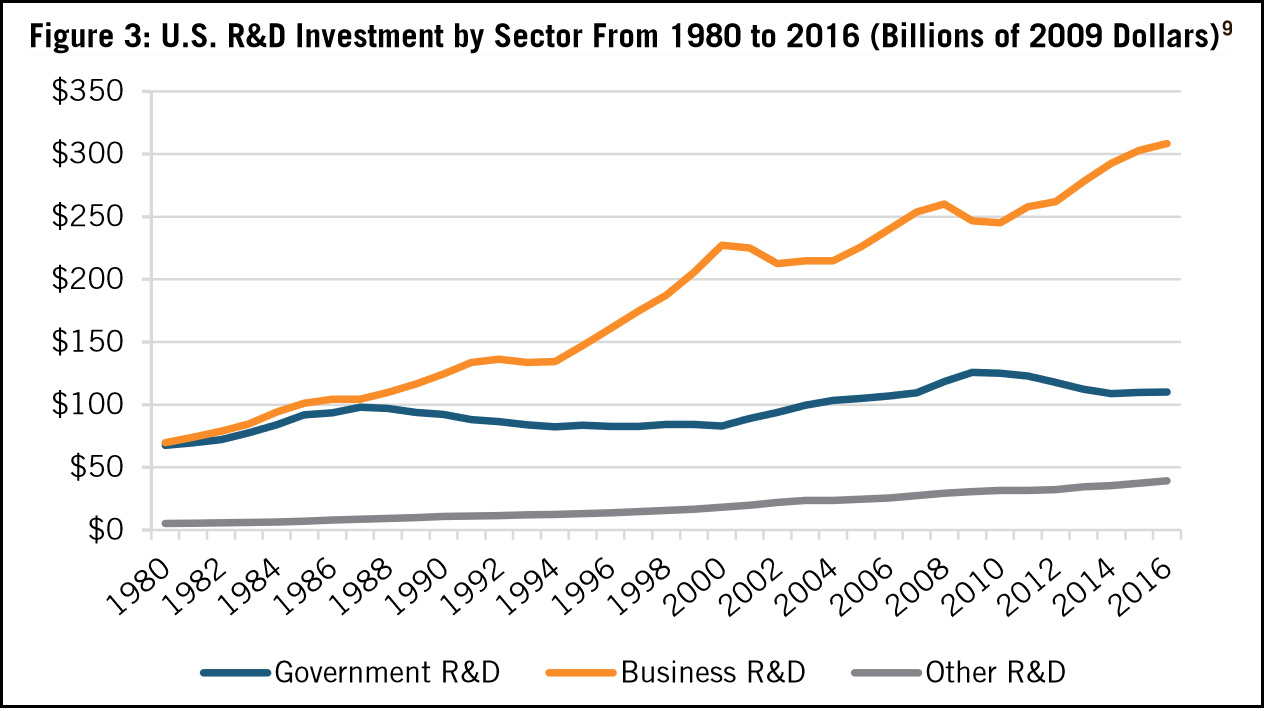
The blue line is the one of interest: it shows federal non-defense R&D spending adjusted for inflation. In the last four decades, it’s gone up from $40 billion per year to nearly $80 billion per year—though it’s been pretty flat since 2003. Still, that’s a sizeable increase. Here’s a related chart:
The absolute numbers are a little different here thanks to a different baseline for inflation adjustment, and the report I took this from explains some of the reasons to discount the business spending growth a bit. Even taking that into account, though, the overall verdict is obvious: government R&D has gone up somewhat while business R&D has skyrocketed from $70 billion per year to $300 billion per year. Put everything together and total US R&D spending has increased from about $140 billion in 1980 to $460 billion in 2016. That’s pretty big growth.
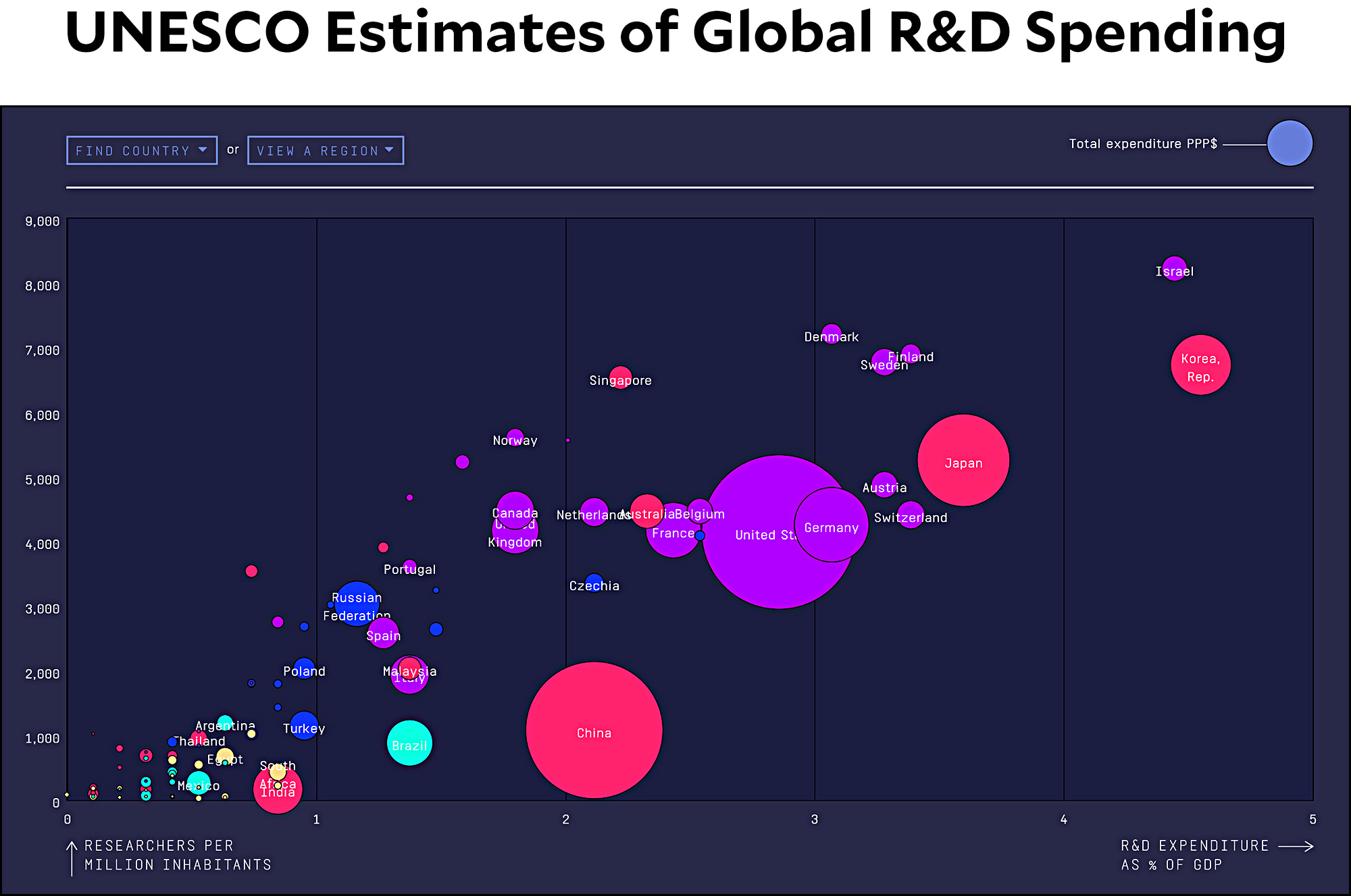
Should we be spending more? You can make that argument. At the same time, we’re obviously not laggards. Our absolute spending is huge, and there are only a couple of countries that are substantially ahead of us in R&D spending as a percent of GDP.
Now, all this said, there are questions about what we spend our money on. How much is for basic research? How much is wasted? Does business R&D spending really serve the same purpose as government R&D spending?
At the same time, I think you also need to look at spending priorities over time. In the past, we spent a lot of money on things that required gigantic investments in physical infrastructure: supercolliders for particle physics, manned missions to the moon, new energy sources, and so forth. Today our interests have moved into areas like genetic editing and artificial intelligence. This stuff isn’t cheap, but it’s inherently less expensive than some of our previous ambitions.
Bottom line: my pushback against the general theme of stagnation has been the same for a long time. We are disappointed that we lack the spectacular physical inventions that we dreamed of in the past: flying cars, lunar cities, and so forth. And I’ll concede that right now we seem to be in sort of an innovation valley. The two biggest areas of near-future progress are almost certain to be genetic engineering and artificial intelligence, and someday those will blow the doors off anything we’ve done before. However, neither one has really delivered yet. Still, it also took a long time for cars and radio and TCP/IP to change our lives after they were first invented. But eventually they did, and so will genes and silicon.
Here’s the coronavirus death toll through April 25. Germany and the United States have both been plateaued for nearly two weeks. When will they start to decline?
The raw data from Johns Hopkins is here. The COVID Tracking Project is here. The Public Health Agency of Sweden is here.
Yesterday I passed along news of a controversy concerning hypertension and COVID-19. The question was simple: does hypertension make COVID-19 more deadly, or is it hypertension drugs that make it more deadly? A couple of new studies out of China suggest that it really is hypertension after all:
One study looked at 362 patients with high blood pressure treated at Central Hospital of Wuhan, the city where the initial outbreak occurred. It found no difference between those on the drugs and those not in terms of the severity of the disease and whether a patient survived or died, researchers from the hospital report online April 23 in JAMA Cardiology. The other study followed 1,128 COVID-19 patients with hypertension from nine hospitals in Hubei Provence, where Wuhan is located. It found that the mortality rate was lower for the 188 on the drugs, an international research team reports online April 17 in Circulation Research.
The new studies provide reassurance that the drugs “are not associated with harm in patients with COVID-19, as some had suspected,” says cardiologist Scott Solomon of Brigham and Women’s Hospital and Harvard Medical School in Boston. But without randomized controlled trials, in which patients are randomly chosen to take a drug or a placebo, “it will be very difficult to get at the truth” of exactly what impact the drugs have, he says.
Sure, we would all like a bunch of randomized controlled trials, but we’re not going to get them in the middle of a pandemic. Observational studies like these are the best we’re going to do, and properly conducted they should provide pretty reliable results. My only hesitation here is that a lot of studies and projections based on the Wuhan outbreak have later turned out to be unique to Wuhan. I can’t think of any reason this should be true for hypertension drugs, but COVID-19 is a weird disease. You never know.
For now, though, this is the best we’ve got. Talk to your doctor, of course, but it looks like hypertension drugs are probably in the clear.
Here’s the coronavirus death toll through April 24. No big changes from yesterday. One comment, though: Canada has been the best performer among my set of countries, but so far it still hasn’t shown any signs of peaking. It may be growing more slowly than other countries, but unless it starts to plateau soon it will end up not much different by the time summer starts.
The raw data from Johns Hopkins is here. The COVID Tracking Project is here. The Public Health Agency of Sweden is here.
Like millions of other middle-aged guys, I have high blood pressure. This is a problem:
Scientists are baffled by how the coronavirus attacks the body — killing many patients while barely affecting others. But some are tantalized by a clue: A disproportionate number of patients hospitalized by COVID-19, the disease caused by the virus, have high blood pressure….An April 8 report by the U.S. Centers for Disease Control and Prevention showed that 72% of hospitalized COVID-19 patients 65 or older had hypertension.
Luckily for me, my hypertension is well controlled using a small dose of an ACE inhibitor called Zestril. So I should be in pretty—
Researchers agree that [hypertension] drugs affect the same pathways that the novel coronavirus takes to enter the lungs and heart. They differ on whether those drugs open the door to the virus or protect against it….The drugs are known as ACE inhibitors and ARBs, broad categories that include Vasotec, Valsartan, Irbesartan, as well as their generic versions. In a recent interview with a medical journal, Anthony Fauci — the U.S. government’s top infectious disease expert — cited a report showing similarly high rates of hypertension among COVID-19 patients who died in Italy and suggested the medicines, rather than the underlying condition, may act as an accelerant for the virus.
Well, that’s just great. Option 1: Hypertension makes the coronavirus more deadly, so take your meds! Option 2: No, it’s the meds that make the coronavirus more deadly, so stop taking them right away!
I would like someone to figure this out very quickly. Thank you.
UPDATE: A couple of studies out of China suggest that hypertension really is at fault, not hypertension drugs. More here.
This is what things look like when we settle into bed for the night. Hilbert adores Marian and pretty much follows her around all day. At night, he jumps up on her stomach and starts begging to be brushed. Sometimes he gets it, sometimes he doesn’t.
I have no special reason for posting this aside from occasional requests to do so, but here’s a couple of charts for US states that are similar to the country charts I put up every morning. First up is a selection of states with a high incidence of COVID-19:
And here’s a selection of states with a low incidence of COVID-19:
New York has clearly peaked and is now headed down. A few other states (New Jersey, Louisiana, Texas, Tennessee) show signs of peaking, but it’s a little too early to say for sure. Others are still heading steadily upward. Overall, I can’t say that this looks especially promising. I wouldn’t be surprised if the overall US number stays plateaued for a while.
Can you pitch in a few bucks to help fund Mother Jones' investigative journalism? We're a nonprofit (so it's tax-deductible), and reader support makes up about two-thirds of our budget.
We noticed you have an ad blocker on. Can you pitch in a few bucks to help fund Mother Jones' investigative journalism?
Billionaires own the media, but they don’t own us.
At Mother Jones we know these aren’t conventional times, and they require unconventional coverage. That’s what we deliver every day: fierce, independent journalism you can’t find elsewhere. Perhaps never in the history of our country has that been more necessary than now. But we can’t do it without reader support—your support. Please chip in today.
Billionaires own the media, but they don’t own us.
At Mother Jones we know these aren’t conventional times, and they require unconventional coverage. That’s what we deliver every day: fierce, independent journalism you can’t find elsewhere. Perhaps never in the history of our country has that been more necessary than now. But we can’t do it without reader support—your support. Please chip in today.